

Whack-a-Mole
Trusting our process when prostate cancer rears its ugly head…again


Rest Stop
Steve and I were two and a half hours into our drive down the coast from our home in Avila Beach to our job site for the day in Manhattan Beach. This has become a very familiar path for us since we made the move to the Central Coast three years ago and since still have clients in the South Bay.

The first part of the drive is usually dark and foggy. When the sun rises, we see dancing vineyards and emerald pastures, then the ocean makes its dramatic entrance on the right as we continue South, the sun slanting brilliance into our eyes. A clean windshield and sunglasses are essential, we have learned.
When we drive together, we talk—a lot. Mostly work and family. Get Steve started on anthropology, AI, the animal kingdom, or any of Yuval Harari’s last two books, and you’re unlikely to get a word in for miles. We also talk about tennis—lots of tennis.
And for the last two years, a big topic, of course, has been prostate cancer. But today, I don’t bring it up.
There’s a Starbucks in a strip mall in Malibu that checks all the rest-stop boxes: easy parking, usually quiet with no line for coffee and no wait for the bathroom. Steve often sits in the parking lot while I go inside. My need for caffeine and my pull toward the restroom are usually more urgent than his.
“Have you checked the portal yet?” I venture to ask as I open the passenger door of the Honda that we seem to spend more time in than our own living room lately.
“I should do that,” he says, his phone already in his hand.
I unfold out of the car and walk stiffly across the parking lot, my legs aching after the long drive. As soon as I pull open the cream-colored door, the supple smell of Starbucks coffee intermingled with sugary baked goods, refrigerated plastic wrappers, and just a hint of the high-octane cleaner they must use disorients me.
I try not to think about the lab results. They may not even be up on his portal yet. But they might. Yet another challenge of being the spouse—I can’t access his medical portal. He controls the timing and the delivery of that information. As he should. But still.
The next part of our drive, I realize, may have a very different tone.
I order my tall coffee in a grande cup so there’s room for cream, and ask for the bathroom code. It’s one of the darker Starbucks, probably because it’s tucked into a corner. As I walk past the packaged goodies, I think that if you asked someone to picture a Starbucks in Malibu, they’d imagine a sun-drenched cafe packed with beautiful models with perfect teeth and lifeguard bodies–the kind of people we cast in our videos, the kind of people who, it would seem, never have to worry about their PSA numbers. They’d be wrong.
Troubling Doubling
Steve was diagnosed two years ago with advanced prostate cancer. He had a PI-RADS 5 tumor taking up almost half of his prostate and the cancer had spread to three lymph nodes. After extensive research, we chose brachytherapy and SBRT (Stereotactic Body Radiation Therapy), and it worked.
His PSA dropped steadily for over a year, hitting a baseline of 0.083 in July 2025. Essentially undetectable. Victory!
This is the part where I remind you that we are NOT doctors and not giving medical advice-just sharing what worked for us and hoping it helps other couples out there.
For nearly a year we had been allowed to return to “normal.” Steve was feeling great and playing tennis more than ever. There were side effects to the treatment we were learning to live with, but not nearly what we believe they would’ve been if we’d taken a more traditional path that included surgery and two years of Androgen Deprivation Therapy (ADT).
All things considered, we were very okay with the “new normal” we got. We went days and weeks without even thinking about it. Things looked so good, we “graduated” down to six-month PSA monitoring.
Then in November, his PSA bumped up a little, to 0.212. No need to panic, but we decided to go back to two-month monitoring. We checked in January and it had doubled to 0.479. By February it was 0.760, and in March, 1.229.
The PSA doubling time was, well, troubling.
As the partner, it’s hard to know what to feel. These monthly PSA tests are important, but so much life goes on in between, and it’s like that mobile phone commercial. Should I be worried now? How about now?
By February, when the numbers continued to rise, we were in action mode.
The R Word
We are dealing with very aggressive cancer, so we had known this was likely to happen. Still, it’s not what you want. You want to be able to say the other C-word…not Cancer, but Cure. And oh, I wanted to say Cure.
Instead it was looking more like the R word: Recurrence.
The word recurrence is problematic in many ways. Recurrence means to occur again. And yet I don’t often hear it applied to good things. You never hear people say, “Gee, I’ve had a recurrence of winning the lottery lately,” or “I’ve had a real good-hair-day recurrence lately.” You certainly never hear anyone talking about a recurrence of good health.
As we’ve learned, recurrence is also not always an accurate word, either, in the case of prostate cancer. Because in many cases, the cancer is not reoccurring. It’s just that some microscopic or MRI-invisible lesions outside of the treatment areas went undetected or missed, and the cancer had a chance to grow into its full evil potential. Not occurring again, just occurring where you can see it.
Even the highly effective PSMA PET scan has a detection limit of under 30% if your PSA is 0.2 or lower.
Blast From the Past
On our first date sixteen years ago, one of the things we bonded over was the fact that Steve had been one of the founders of Blast Radius, an internet startup. “No way,” I said when he told me. “I worked for USWeb. We hated you guys.”
We were sitting on brown Adirondack chairs on the back patio of what has to be one of the most beautiful Starbucks ever built: the one at Golden Cove Plaza on the Palos Verdes Peninsula. Don’t take my word for it-check out the view here:
Not a bad first date, reclining next to cement fire pits overlooking the Pacific as far as Catalina Island on a clear day. Little did I know then that I was staring at our future wedding venue.
There were a million startups back then, but our respective companies went toe to toe on some of the biggest brands out there: Nike, NBC, Sony, Nintendo, Universal, Casio. I remember my USWeb team burning the midnight oil to prepare the best, most creative pitch we could–trendy Flash homepages, kick-ass creative concepts, every multimedia trick in the book. This was the same thing most of the other agencies did.
Except Blast Radius. They pitched process.
Steve’s team showed cool, cutting-edge work or their own, but refused to guess what a new client might want or need. My team got lucky sometimes and won on talent alone, but what we failed to recognize was that creative is driven by business goals and strategy. Steve’s team knew that. They promised a mind-blowing creative product (and had the awards to prove it), but only if the client followed their strategic planning process first. And they won…a lot.
Our coffee grew cold, the air grew colder, and we kept talking about the dot-com days. I was vaguely aware the babysitter was probably going into overtime, but even back then, Steve and I found it easy to talk to each other.
Not long after our relationship got serious, Steve told me, “If we’re going to make this work, we are going to need to work together.” He meant it literally—otherwise we’d both be working really hard for other companies and never see each other. So our little business was born. And that’s how I learned, up close, what made Blast Radius so successful.
The Man with the Plan
Fast-forward to Steve’s cancer treatment. With so much uncertainty, it really helps him to feel more in control when he can use the tools he trusts—strategy and process—just like we do in business.
In this case, though, instead of building a website or making a video, he was devising more of a war plan. His body had been invaded and we had to research the enemy and make a plan to drive it out.
First, we used the best diagnostic tests to determine what we were dealing with: PSA tests to flag the issue in the first place, MRIs and PSMA PET scans to see where the little cancer critters were hiding, then the treatment itself, and then a plan to catch anything we didn’t get the first time.
So this was the post-treatment plan:
Test PSA regularly.
Three rising PSAs, and we go back for a PSMA PET scan.
In order for this plan to work we needed accurate PSA results, which ruled out ongoing Androgen Deprivation Therapy.
A.D.T. N-O-T
Steve had used ADT only for six months during his initial treatment. He started with Casodex, then Lupron, and Abiraterone concurrently (the latter nearly landed him on the list for a liver transplant).
He’d agreed to ADT (but only in the short term) to suppress the cancer’s growth while we waited for approvals, and to shrink the index tumor away from the neurovascular bundle, rectal wall and urethra before brachytherapy—creating a wider margin, thus lessening the risk of radiation damage.
ADT was a miserable experience. I’ve never seen Steve so weak, tired, and depressed. Hot flashes. Poor sleep. He just wasn’t himself. Abiraterone can also cause liver injury, elevating liver enzymes, and in rare cases, liver failure. Luckily our local oncologist detected this issue at the three-month blood draw, and caught the problem before his liver failed (although not without a nerve-wracking trip to the ER!).
So when Steve’s doctors advised him to stay on ADT (as standard of care) for 18-24 month after his initial treatment, he went deep into research. Multiple respected urologists gave several reasons not to:
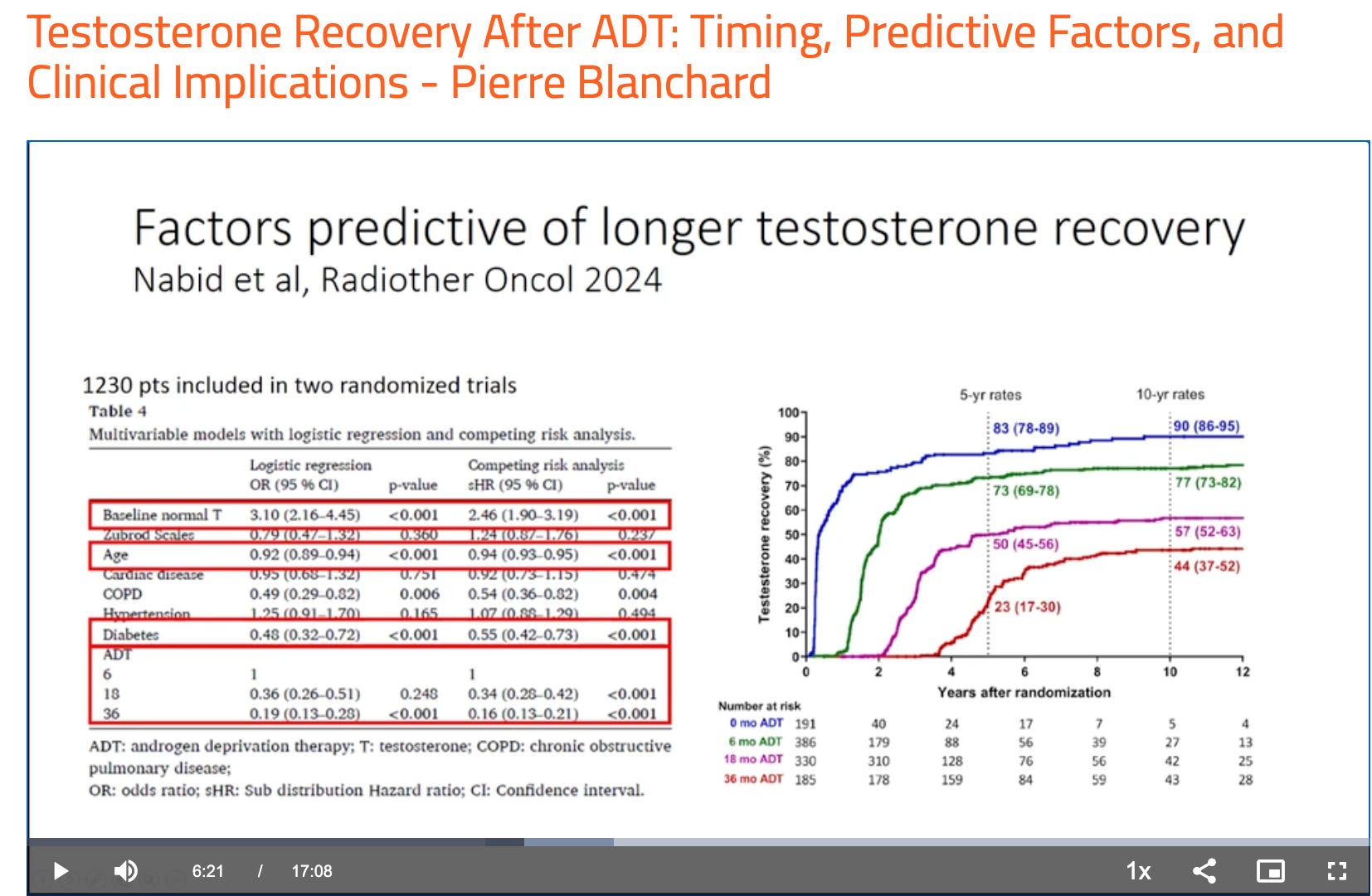
1. If you stop your testosterone for too long (and no one knows exactly how long that is for each person) it may not come back. We definitely wanted it back.
“Many of the patients who had longer duration of ADT never actually recover that testosterone.” - Pierre Blanchard, MD, PhD, Professor of Radiation Oncology, Institut de Cancérologie, Gustave Roussy Cancer Center, Villejuif, France
2. Studies have shown similar outcomes between patients who stayed on ADT after treatment and those who did not.

3. Perhaps most importantly: if you suppress testosterone, you artificially lower your PSA. PSA monitoring is the canary in the coal mine of prostate cancer recurrence detection post-treatment. If you can’t monitor PSA, you don’t know whether the cancer has come back.
“PSA is an androgen-dependent molecule. That means that you need testosterone in order to make PSA. If your testosterone level is so low that you can’t make PSA, when we’re routinely following and checking patients for PSA, you have a falsely low PSA that you’re looking at.” Bernie HL. Testosterone and Prostate Cancer: From Dogma to Data. Grand Rounds in Urology. February 2026. Accessed Jul 2026. (⬅️ Great video!)
Remember my USWeb days? I wasn’t in business development like Steve. I was a producer in the creative department, and often had to write up status updates for clients who were shelling out big bucks and wanted to know they were getting their money’s worth. A big part of that process is metrics. How many clicks did my email campaign get? How many impressions on my landing page? How many views of my Superbowl ad?
Bottom line is: there’s no way to know if you’re successful if you don’t have a way to measure. Taking away testosterone in this case takes away your ability to get reliable data.
Here’s more we have written about the role of testosterone and PSA.
Deja Vu
So the PSA was rising and his testosterone was above the normal range, we knew the cancer meant business. It was time to get to work.
A lot had changed in the two years since initial treatment. As an example, PSMA PET scans were now available in our little city; before, we’d had to drive down to UCLA.
And yet most things had not changed. The same medical facilities, the same hold music, the same slog to get approvals pushed through insurance, the same waiting game.
We saw the local oncologist and we all agreed the PSMA PET scan was the obvious next step. We’ve written about the magical PSMA PET scan before, but I’ll say it again: this is the technology that has let us pursue such an aggressive strategy with so much confidence. And it did not disappoint.
We weren’t surprised that cancer was detected, but we were relieved to see that only one area lit up: the posterior cortex of the S1 sacrum. The bad news: that’s a bone metastasis.
We had to act quickly and carefully. Steve did what he does best. He went straight to the research. What we found was that the best course of treatment for us was, again, SBRT.
Our oncologist agreed, but couldn’t refer us to a radiologist without getting more detail from an MRI first, which meant several calls back and forth with the doctor’s office and referral coordinators, chasing down approvals, until we finally pushed it through.
The MRI confirmed the diagnosis, and the news was as good as this kind of news gets: we were catching the bone met very early, before it had done any real damage.
We went back to our original trusted radiologist–the one who’d done the brachytherapy. SBRT to the sacrum, we were told, is generally straightforward since that part of the body doesn’t move much. But we were still nervous. The sacrum houses nerves that control the lower body–nerves that matter to anyone who cares about walking, and especially to an avid tennis player like Steve.
We will talk more about SBRT in another post, but suffice it to say it’s a medical miracle. Three 15-minute visits, no pain, lots of gain.
And just like that, we’re back to phase 1 of the plan: PSA testing.
How Low Can You Go?
Back at the Malibu Starbucks, I grab my coffee and dump in a healthy pour of creamer. They have apparently changed their design—same bleached white waxy cardboard cup, but the tops are some kind of recycled cardboard now. It takes real muscle to remove, and once it’s been pried off and the cream applied, it doesn’t want to go back on in any way that seals the liquid inside with confidence. But hey, it’s better for the environment and probably us, so all good.
I take a sip on the way out through the parking lot, and instead of that satisfying “first-sip feeling,” the lid slips and I get hot coffee sloshed onto my thighs. I pull open the car door and lower myself clumsily into the seat without spilling further, explaining the awkward splotches on my jeans.
And then I see the smile on my husband’s face. He holds his phone out for me to read. From the scrolling, I can tell he’s already had a decently long conversation with his AI app while I was inside. I don’t have my glasses on, so all I can make out is “Outstanding results,” but I don’t really need to read the rest. The look of relief and happiness on Steve’s face tells me all I need to know: the PSA is back down! He explains it’s not just down, it’s 78% down from where it was before this round of SBRT.
I don’t like to let AI put words in my mouth, but I have to agree this is truly “outstanding” news.
Trust the Process
That low PSA number confirms that spot on the sacrum was the source of the rising PSA—and we got that little cancer gremlin 👿—it also affirms there are no other tumors currently emitting PSA.
I’ll drink ☕️ to that!
Of course, we’ll also stay vigilant and keep our Whack-a-Mole hammer handy. 🔨
Steve’s Post-Treatment Plan*
Test PSA each month (same day if possible).
Stay off androgen deprivation therapy so PSA levels are as accurate as possible. Don’t be afraid of testosterone!
If the PSA rises two times in a row or PSA doubling time is fast, work with your oncologist to schedule a PSMA PET scan.
Research and evaluate your treatment options with your team (your oncologist, primary care doctor, etc. - and of course your partner 💕) Here’s our post about finding online experts you can trust.
Treat the cancer (If oligometastatic, SBRT is probably a good bet, but check with your doctor).
Whack-a-mole and repeat as needed.
*This is Steve’s plan. Steve is not a doctor. This is working for us, and we are sharing it as an example of how researching and working with your doctor can work. We’re also sharing our journey as a couple, since prostate cancer is often referred to as a couples’ disease and we are in this together. We hope it helps you and your loved ones. ❤️
Brenna
Happy for you. Ever notice they talk about tests, and how to fix, but hardly ever mention how to prevent in the first place. Since I started taking Salvestrol, my PSA has dropped from 8.5 to under 3. The lesion seen and biopsied disappeared. Will have another MRI and PSA tests done beginning of September. All my doctors said Salvestrol would not help, but none can explain the results. Before retiring my main doctor said, whatever you are doing, keep doing. I go to a Prostate cancer survivors meeting once a month and most of the men have had a lot done. Primarily by the time they discovered the cancer it had already spread.